We're on a roll with parasites in muscle biopsies! Here is one from my archives. No history, but the findings are classic. Diagnosis? How is this different from the muscle parasites in the last 2 cases?


We're on a roll with parasites in muscle biopsies! Here is one from my archives. No history, but the findings are classic. Diagnosis? How is this different from the muscle parasites in the last 2 cases?
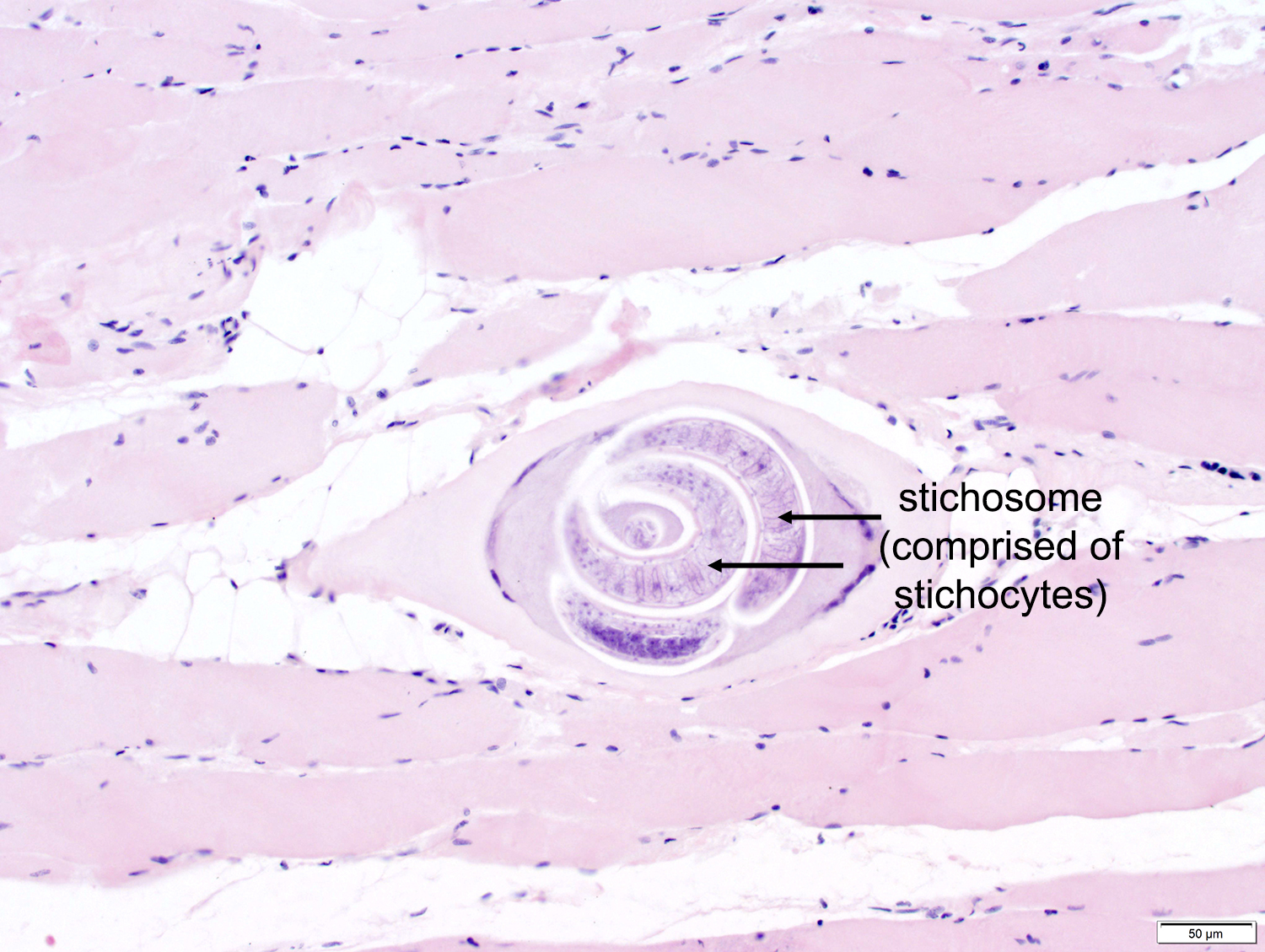
Answer to the Parasite Case of the Week 708: Trichinella sp. larva; coiled within a muscle "nurse cell". Larvae are the only form seen in muscle with this infection. Compare this to our recent case of Haycocknema perplexum infection in which gravid female worms were seen 'crawling' through the muscle fibers. These two helminths are also quite different than muscle infection with the protozoan parasite, Sarcocystis, as shown in Case 707. Keep an eye our for our next case that will show a very different parasite in muscle!
Trichinella sp. larva within muscle:


This week's case features another muscle biopsy - this time from a middle aged man from China with recent visit to Pangkor island. Approximately 10 days after his trip, he presented with high fever, headache, and generalized myalgia. Light microscopic evaluation of H&E-stained sections of muscle showed the following parasites within muscle fibers. What is your diagnosis?


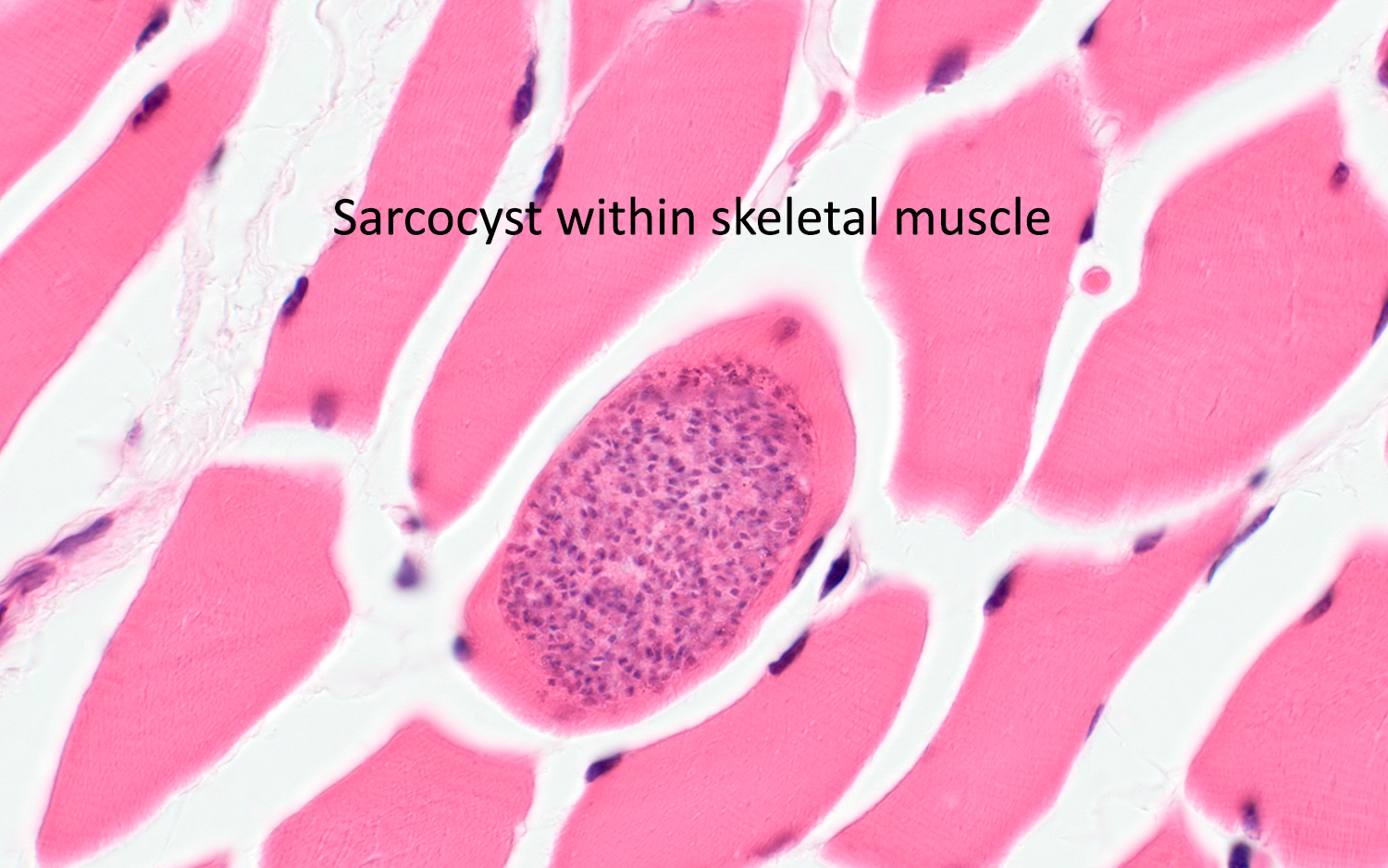
Answer to the Parasite Case of the Week 707: Sarcocystis species. Molecular testing is required for identification of the causative species.
This case shows a single intramuscular sarcocyst containing multiple bradyzoites. The clinical history and epidemiology also supports a diagnosis of sarcocystosis.
Many of you rightly suggested that the differential diagnosis includes Toxoplasma gondii, a related apicomplexan parasite which can form similar-appearing cysts in tissues throughout the body. Toxoplasmosis involving skeletal muscle is seen primarily in profoundly immunocompromised individuals with widely disseminated disease. When T. gondii is in the clinical diagnosis, then species-specific immunohistochemistry and/or PCR can be used to confirm the diagnosis.
Happy New Year! I thought I'd kick off the year with a fascinating and enigmatic parasite that can cause very rare but devastating disease in humans. The patient is a man in his late 30's who presented with 8 years of progressive weakness, significant weight loss (>30 kg), dysphagia, and dysphonia. His creatine kinase levels were elevated and he had peripheral eosinophilia. He was previously healthy prior to the onset of symptoms, but was wheel-chair bound on presentation. The patient had spent a significant amount of time in the bush regions of coastal northern Queensland, Australia.
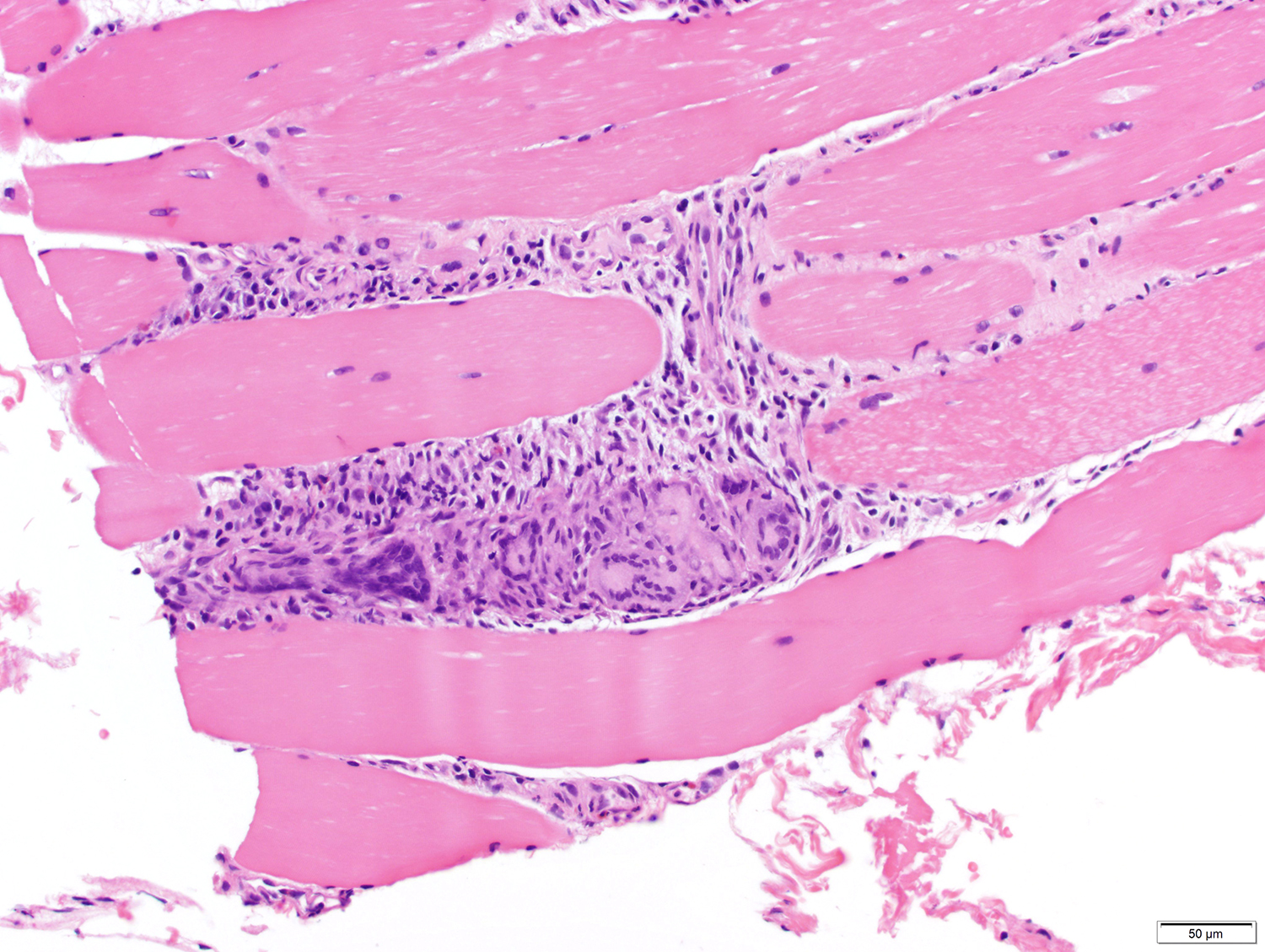
Muscle biopsy revealed muscle damage and extensive accompanying lymphoplasmacytic and granulomatous inflammation, as well as the rare parasites within muscle fibers.
Inflammation and muscle damage:

Parasites (click on images to enlarge and see the diagnostic detail):


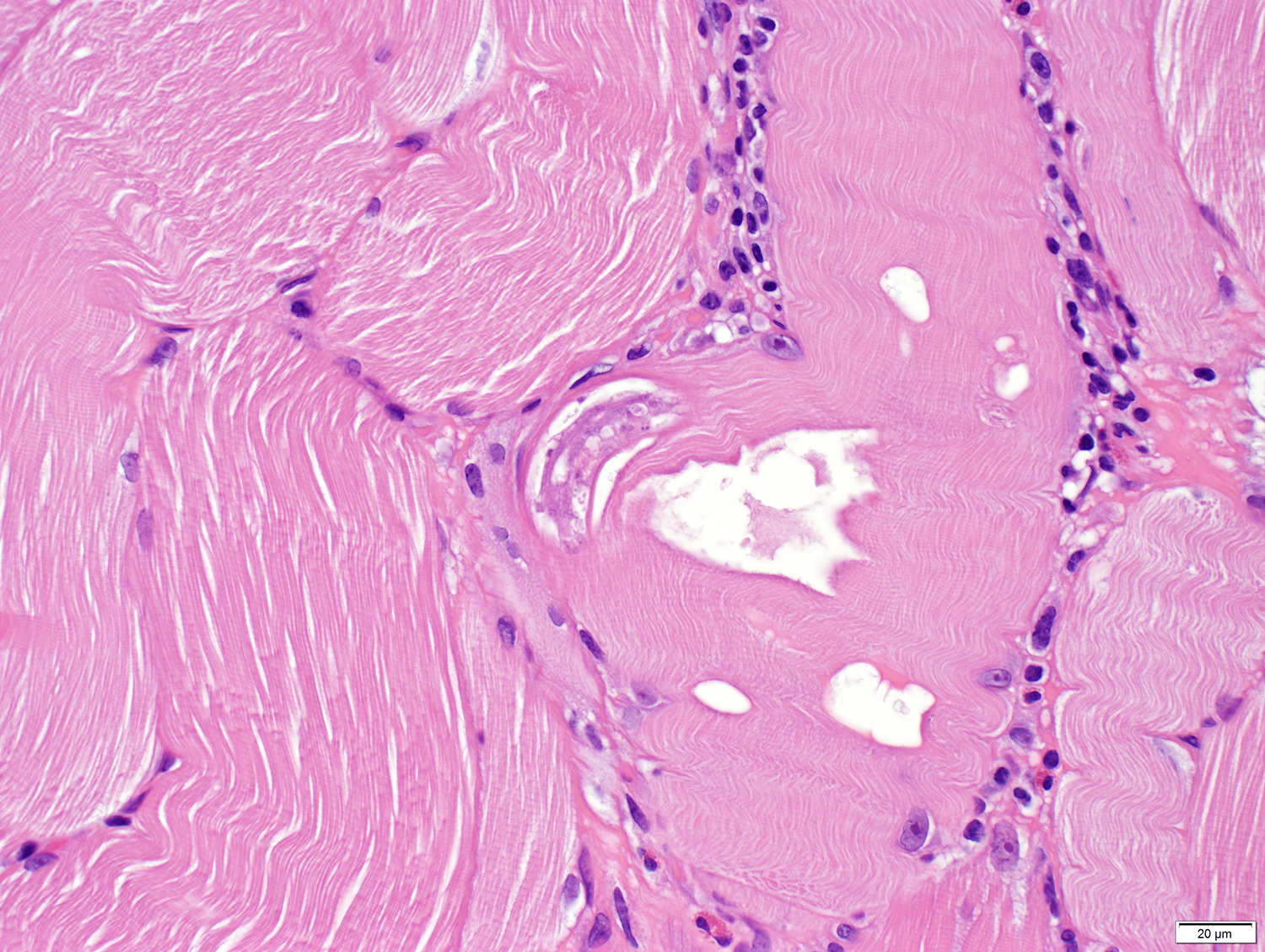


Identification? What is your differential diagnosis?
Answer to the Parasite Case of the Week 706: Haycocknema perplexum infection
Wow, I am so impressed by the responses on this case! There are many helpful comments and links in the comment section of this blog which you may want to check out.
Haycocknema perplexum infection (haycocknematosis) is an extremely rare parasitic infection. There have only been 13 humans cases (including this one) reported to date. As Florida Fan noted, Blaine and I previously presented this case as a poster, and it has now been published in Emerging Infectious Diseases. You can read the article HERE. The article describes the diagnostic features of this nematode in histologic sections, including the presence of adult females containing fertilized eggs. I included a photo of one such female in this case as it played a key component in the diagnosis.

Note the presence of numerous (8-12) eggs (arrows) within the body of the female in this image. These eggs will hatch within the female, develop to 3rd stage larvae, and then burst through the head of the female, killing her in the process (yikes!) The larvae will mature into male or female worms within the muscle, and these will then mate and propagate the infection. This allows the infection to last for years (and potentially for the life of the host).
As noted by Nema, it is very important to differentiate this infection with trichinellosis (a.k.a. trichinosis), as the prognosis and treatment are very different. While both nematodes infect striated muscle throughout the body, the following are important features that allow for differentiation of haycocknematosis and trichinellosis:


