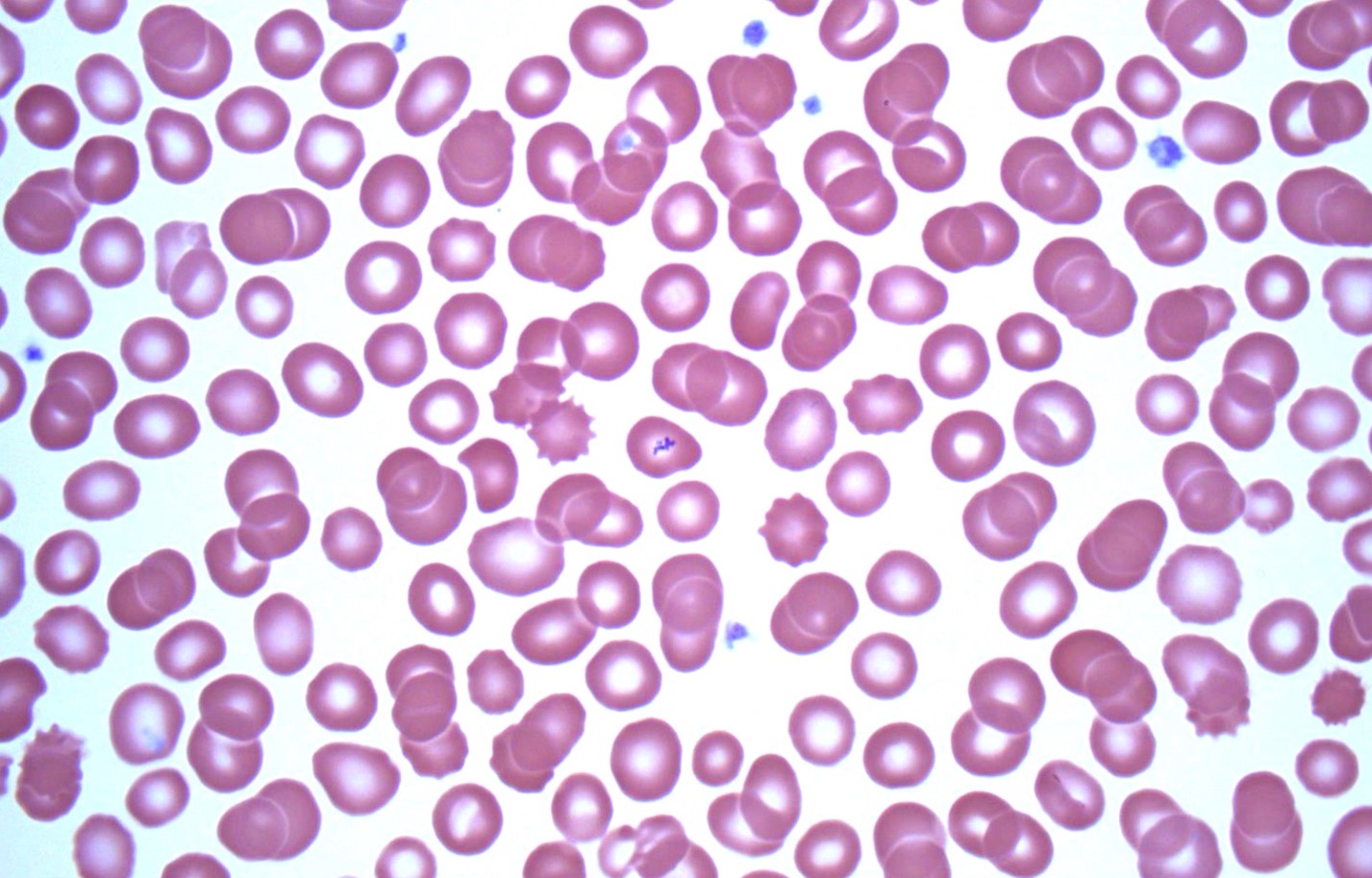
This week's case features some objects on unstained wet preparations of whole blood. What are we seeing here? How do you process blood specimens in your laboratory for this type of organism?
Monday, August 19, 2024
Sunday, August 18, 2024
Answer to Case 755
Answer to the Parasite Case of the Week 755: microfilariae; permanent staining needed for further identification.
I'd like to give a giant shout out to the Filariasis Research Reagent Resource Center (FR3) which provided this specimen to me for a course I was teaching - the first annual Mayo Clinic Parasitology Workshop. The live microfilariae were a big hit with my course attendees, so I wanted to share the specimen with all of you as well! This particular sample contained Brugia pahangi (orderable through BEI: NR-48896).
Thanks to all of you who wrote in to share your diagnostic protocols for the microfilariae. In my laboratory, we screen all Giemsa-stained thick and thin blood films for microfilariae using the 10x objective before going to higher power. However, like Florida Fan, we offer a specific test for microfilariae when suspected clinically. For the microfilariae test, we request that blood be submitted in 3.2% sodium citrate (light blue topped tube) and then perform a Knott's concentration. We no longer examine fresh wet preps of blood due to the concern for infectious diseases (so seeing the live microfilariae in this 'safe' NIH sample was a real treat for us). The Knott's involves the addition of 2% formalin to the blood which lyses the RBCs and make the microfilariae easier to identify. We then centrifuge the specimen and make Giemsa-stained, methanol-fixed smears for examination.
You can read more about the human infecting microfilariae found in blood in a paper I wrote with Blaine Mathison and Marc Couturier HERE. There is a nice algorithm for differentiating the various species. Enjoy!
Tuesday, August 6, 2024
Case of the Week 754
This week's case was generously donated by Dr. Jacob Rattin. The following objects were seen from Wright-stained thin blood films taken from a middle-aged woman with unexplained fevers. What is your diagnosis?



Monday, August 5, 2024
Answer to Case 754
Answer to Parasite Case of the Week 754: Platelets overlying RBCs, an intraerythrocytic blood parasite mimic. Many thanks to Dr. Jacob Rattin who donated this case and provided the following helpful explanation.
Normal platelets are 1.5-2.5 μm in diameter and are morphologically round-to-oval and granular (Figure 1, arrowheads).

On Wright stain they are usually blue/purple and on Giemsa stain they are normally pink/purple. As seen in Figures 1 through 4 (arrows), platelets can overly red blood cells (RBCs), mimicking a blood parasite (e.g., Babesia or Plasmodium). In Figure 5, the green arrow is pointing to stain precipitate overlying an RBC.




Helpful morphologic clues to differentiate this pitfall from a true parasite are the following:
1. Platelets overlying RBCs often have a “halo” around them which is likely from it pressing down upon the RBC, which signifies it is not actually intraerythrocytic.
2. The platelets lack any definitive morphology of a parasite.
3. Other normal platelets in the field should resemble the platelet/s overlying the RBC (which is apparent in Figures 1 through 5).
4. As always, clinical information integration is crucial! Checking the patient’s medical and travel history can aid in the differential diagnosis.
Subscribe to:
Comments (Atom)


