Welcome to my new readers!
The answer to Case 410 is amebic keratitis due to
Acanthamoeba sp.
As several of you mentioned, this organism can be identified by the presence of both trophozoites and cysts in the patient's specimen, as well as the characteristic source (ocular/contact lens) and exposure history (swimming in fresh water). Both
Acanthamoeba spp. and
Balamuthia mandrillaris form cysts and trophozoites in humans, whereas
Naegleria fowleri only forms trophozoites (and rarely flagellated forms in cerebrospinal fluid), and therefore the latter can be excluded by the presence of the cyst forms. Of the two organisms that do form cysts in humans, only
Acanthamoeba species are known to cause ocular infections - primarily in patients who wear contact lenses, thus giving us our final diagnosis.
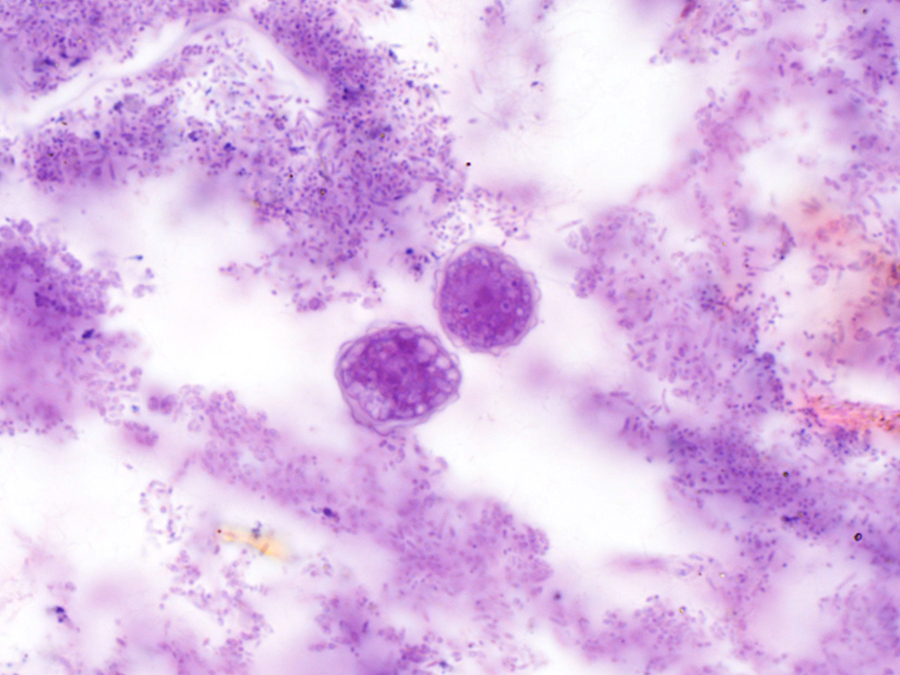
Trophozoite:
Cysts:
Acanthamoeba are free-living amebae that are ubiquitous in fresh water sources and can therefore easily contaminate contact lenses when worn during swimming. Note that there are also abundant bacteria present in this specimen. The bacteria that grew in the routine cultures from this patient were also common environmental organisms, and it is therefore they also likely were introduced while he was swimming with his contact lenses.