Answer to
Parasite Case of the Week:
Strongyloides stercoralis
This is a great teaching case from both the clinical and microbiology standpoint. As many of you pointed out, the clinical presentation is classic for
Strongyloides hyperinfection with eosinophilic "asthma" (likely Loeffler's syndrome due to filariform (L3) larvae leaving the gut and migrating to the lung), receipt of an immunosuppressive agent (which decreases the host's ability to control the infection), and recurrent Gram negative bacteremia. As Harsha mentioned, the "Gram negative bacteria 'piggy back' on the larvae as they autoinfect entering from gut into blood setting up another cycle." This is why patients with hyperinfection syndrome commonly present with recurrent bacteremia and/or meningitis.
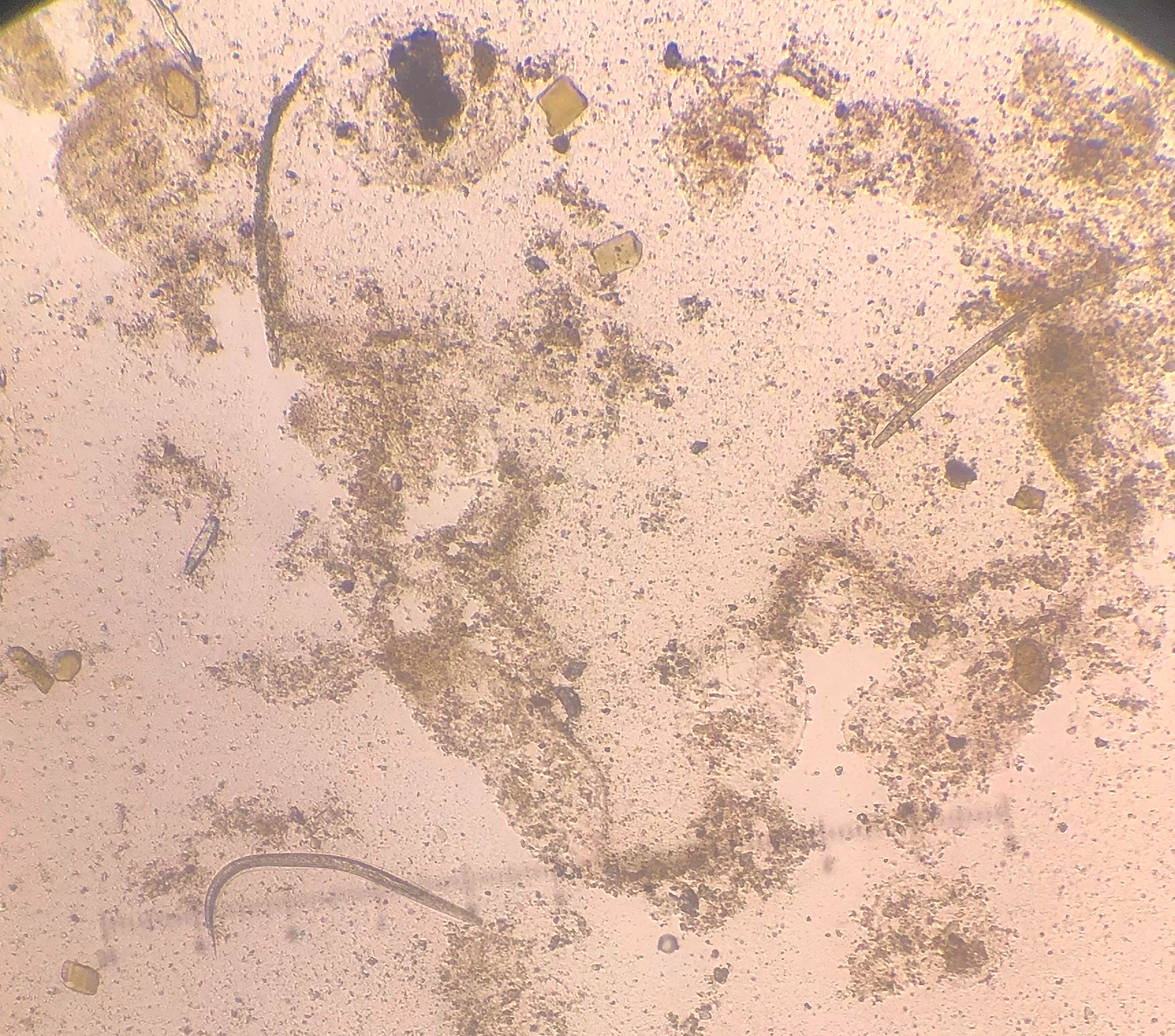
The microbiology findings are also classic. In this impressive case, we see many rhabditiform (L1) larvae in the stool. Filariform (L3) larvae may also be seen, although they are not highlighted in this case. The rhabditiform (L1) larvae of
S. stercoralis have a short buccal canal (think S for strongy, and S for short), which allows them to be differentiated from the L1 larvae of the hookworms (which have a long buccal canal). Hookworm L1 larvae can occasionally be seen in stool specimens when the specimen is not collected into a fixative and is allowed to sit for some time before examination. Therefore, being able to differentiate between hookworm and
S. stercoralis L1 larvae can be important. In this case, you can nicely see the short buccal canal, thus confirming this as
S. stercoralis:
We also have the respiratory findings which support the diagnosis of strongyloidiasis, given that hookworm infection does not produce ongoing respiratory symptoms. Seen here are
S. stercoralis L3 larvae, and also eggs! Presumably the eggs came from adults in the lung, which must have matured from the L3 larvae. Very cool. The bacterial trail from a migrating larva on the blood agar plate is another classic microbiology finding.
On a final note, I'd like to give credit to the astute internal medicine resident, Dr. Guoyou Chen, who thought to order the stool parasite exam based on the clinical findings of eosinophilic "asthma" and Gram negative bacteremia in the setting of immune compromise. Thanks also to Lorraine Sykes and the Microbiology laboratory for contributing this fascinating case!