Happy New Year! I thought I'd kick off the year with a fascinating and enigmatic parasite that can cause very rare but devastating disease in humans. The patient is a man in his late 30's who presented with 8 years of progressive weakness, significant weight loss (>30 kg), dysphagia, and dysphonia. His creatine kinase levels were elevated and he had peripheral eosinophilia. He was previously healthy prior to the onset of symptoms, but was wheel-chair bound on presentation. The patient had spent a significant amount of time in the bush regions of coastal northern Queensland, Australia.
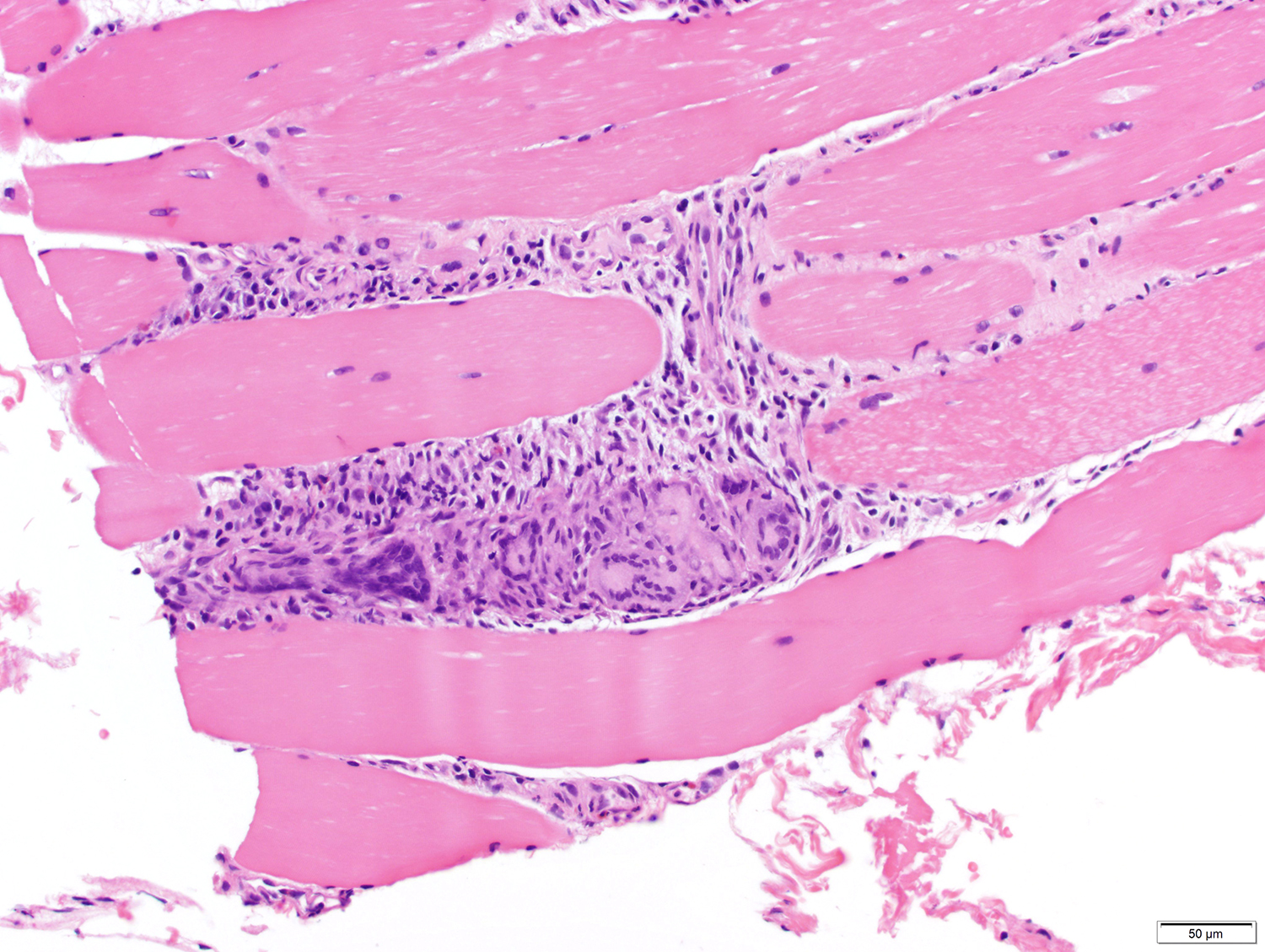
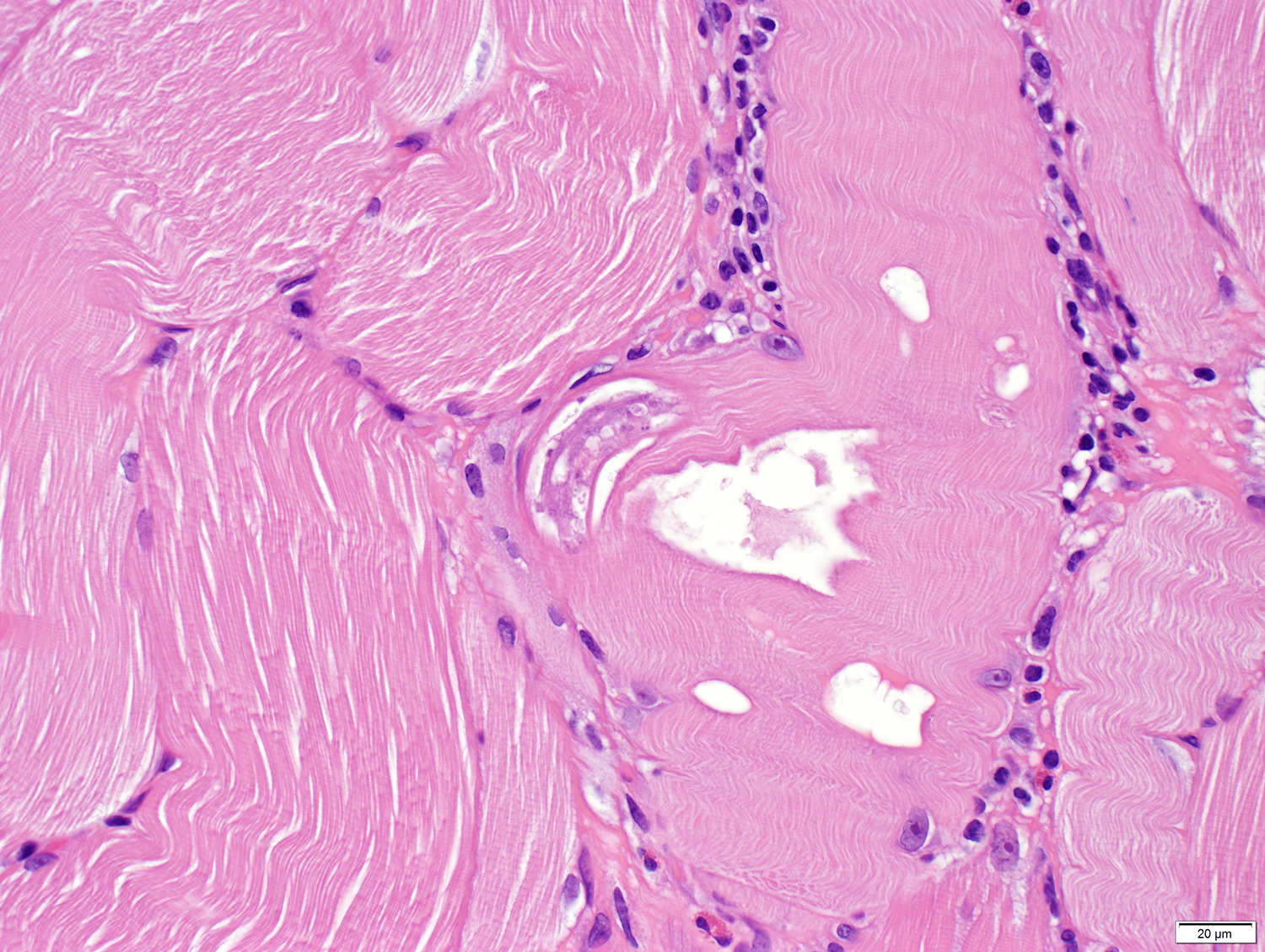
Muscle biopsy revealed muscle damage and extensive accompanying lymphoplasmacytic and granulomatous inflammation, as well as the rare parasites within muscle fibers.
Inflammation and muscle damage:

Parasites (click on images to enlarge and see the diagnostic detail):




Identification? What is your differential diagnosis?



10 comments:
I admit it, “Je n’en sais rien’’ . This is I believe the second experience with this parasite on the Blog. Both times the patients had either sylvatic contact or having been in the bush of Northern Queensland. From this geographic location, my reading led me to articles depicting rare cases of myositis involving Haycocknema perplexum. There is also a poster of the case authored by no one else but Dr. Pritt and Blaine Mathison “Legere est discern”.
Florida Fan
Sorry, once again the auto spelling check mis-corrected the writing. It should be “Legere est discere”
Florida Fan
Thanks for sharing this very rare parasite case. Haycocknema perplexum is my idea too based on symptoms, location and the HE stained sections. Impressive! Not much known about life cycle.
First of all: Happy and healthy 2023 to all the blog readers and especially to Dr. Pritt, who always provides us with the most wonderful challenges that parasitology has to offer! We have learned a lot already and will hopefully continue to do so for a long time to come!
That being said, I have to admit: I was baffled by this case! But as Florida Fan pointed out, the geography and the symptoms all point to a very specific and rare parasite. When looking this one up, the diagnosis is confirmed by the histology images: Haycocknema perplexum infection!
What a beautiful start of the new year! Thanks again Dr. Pritt!
In which case, it is very important to make the differential diagnosis between an infestation by Haycoknema perplexum and one by Trichinella spiralis, a more cosmopolitan and more frequent affection,in which there can also be myositis with hypereosiniphilia but for which the recommended anthelmintic treatment (Albendazole) is of much shorter duration (2 weeks vs 3 months).
We were taught from medical school that "history is king", and I distinctly recall one of our lecturers (a rheumatologist) talking us through a case where a patient presented with muscle weakness, and as the case unfolded and more and more information was provided, it culminated in a biopsy for which the final diagnosis was Haycocknema perplexum infection, same as this. Thank you for this wonderful case!
LS
Haycocknema perplexum
https://neurologyopen.bmj.com/content/4/1/e000290 says :
Conclusions This report aimed to raise awareness of H. perplexum myositis and the possibility of subclinical infection, which suggests a protracted disease course. Further research is required to identify a non-invasive diagnostic test, given that early diagnosis and timely initiation of albendazole treatment may drastically limit patient disability.
Another very intersting source: https://wildlifehealthaustralia.com.au/Portals/0/Documents/FactSheets/Public%20health/Haycocknema%20perplexum.pdf
Some more questions: This species / genus seems to be more known in wild animals- is there done any more research in _Australian animals to culture this "worm" in tissue cultures or do any transfer to other animals with living larvae gained from infested tissues?
Sorry for my bad English - Ulrich > duerr.ulrich@gmx.net
Trying to spezialize on Parasitology about 50 years ago Than spedialised on Eimeria stidai, failing to go further in this section for living circumstances .But newly interested in Parasitology through parasitewonders!
Some comments in answer to Anonymous' question about Haycocknema in Australian wildlife. Although it is assumed that this is a zoonosis from marsupials (with wallabies particularly implicated in several cases), this has not been confirmed. Although associated with wildlife exposure, it remains possible that it could be acquired from environmental sources in forested areas. WE simply don’t know. No one has yet found this nematode in any host other than humans, though some sampling of native wildlife in Australia is now occurring.
The excellent fact sheet from Wildlife Health Australia that was linked is incorrect in one point. Although first described as member of the Muspiceoidea, molecular analysis by Dr Anson Koehler in Prof Robin Gasser’s lab at the University of Melbourne has shown that the phylogenetic positioning of this worm is between the Oxyuridomorpha and the Ascaridomorpha.
To add a further question – why has this infection only been reported as acquired in North and Far North Queensland, and Tasmania? Is this because the parasite is only present in these locations? Is the source of infection is only present in these locations? Or is it simply a factor of greater awareness of this disease among medical staff in those regions?
Certainly a perplexing worm and disease, raising many unanswered questions.
I had no idea what this was, but I do hope that Dr. Pritt's discussion of this case will address what therapies are available for this patient, as well as his prognosis.
Happy New Year to all.
Brenda Waters
Post a Comment