Answer to the Parasite Case of the Week 770: Schistosoma mekongi
The following excellent discussion is by our guest author, Dr. Asra Hasan:
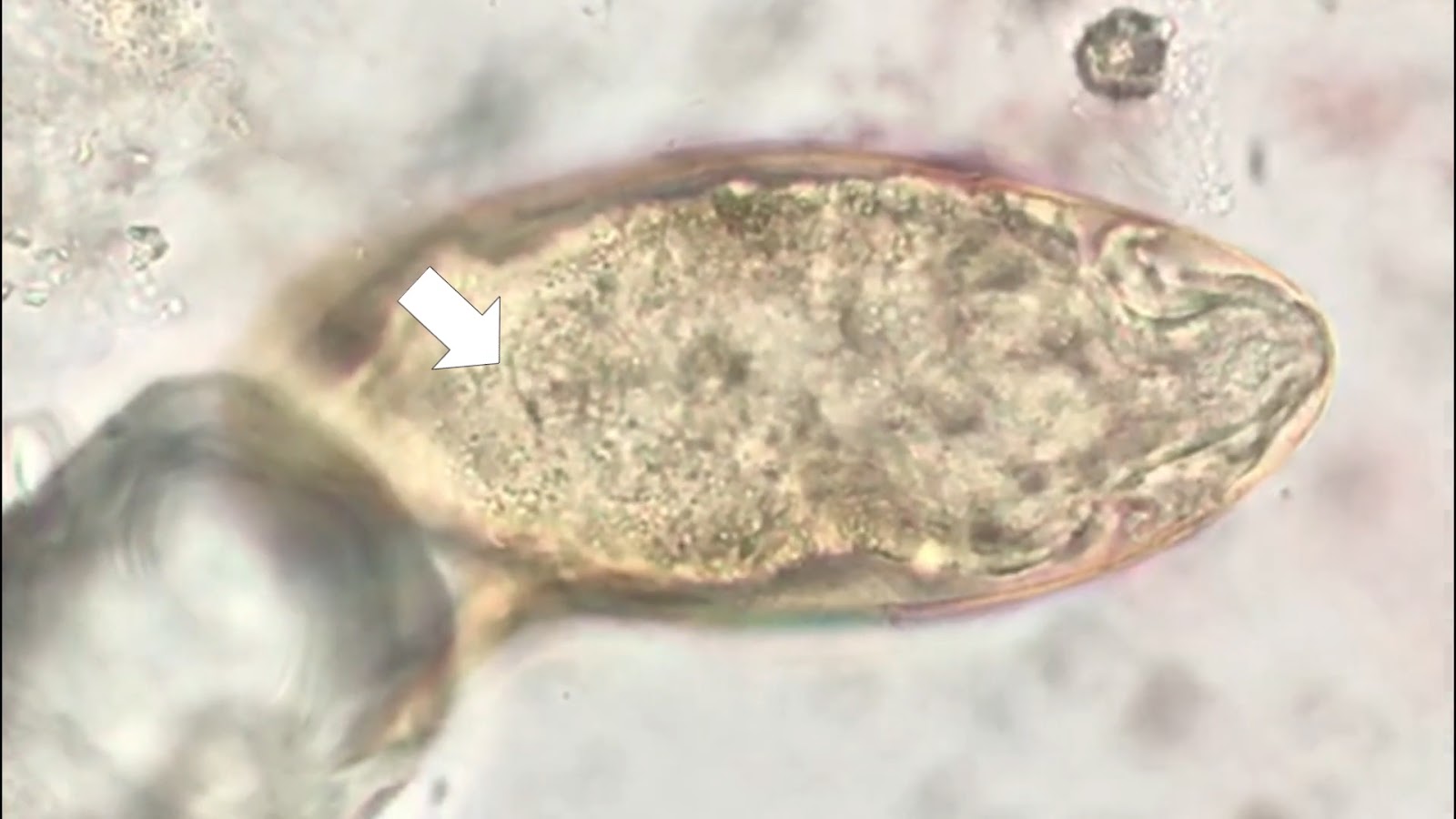
This week’s answer is Schistosoma mekongi! With that, we’ve shown a Schistosoma trio already for the new year—S. haematobium, S. mansoni, and now S. mekongi. Great job, Florida fan! You correctly spotted the inconspicuous lateral spine and the internal miracidium of S. mekongi. And a shoutout to our anonymous writer—your answer was pretty close, as S. mekongi looks a lot like S. japonicum, just smaller, and with a slightly different geographic range.
The endemic area for S. mekongi is along the lower Mekong River—Laos, Thailand, and Cambodia—hence, the population at risk is comparatively smaller than for other Schistosoma species.
Have a read of the clinical vignette below:
“A 42-year-old male rice farmer from a rural village in Cambodia presents to a local clinic with complaints of chronic diarrhea, abdominal pain, and progressive weight loss over the past six months. He also reports intermittent fever and generalized weakness. On examination, he has hepatosplenomegaly and mild ascites. Laboratory results reveal eosinophilia, and stool microscopy shows small, subspherical eggs with a minute lateral spine at one end. The patient has frequent exposure to river water while working in the fields.” And that would qualify as a typical case for this week—S. mekongi!
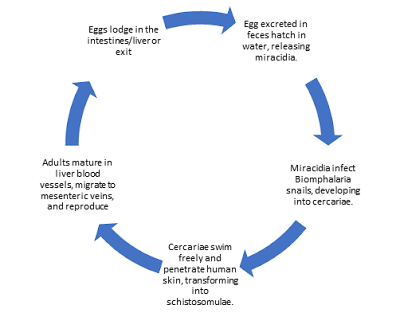
The life cycle is similar to other Schistosoma species discussed on this blog (for example, Case 766), except that the definitive hosts are both humans and dogs, and the intermediate host is the snail Neotricula aperta. S. mekongi primarily affects the intestines, liver, and spleen, and rarely, disseminated sites such as the brain.
Diagnosis
Microscopic examination of stool after sedimentation concentration is used to detect eggs.
Antigen tests: Point-of-care lateral flow assays detecting CCA are used for field screening. In the lab, ELISA has been used to detect circulating schistosome antigens in serum and urine and may be the preferred method for confirming diagnosis. Since stool examination can detect schistosome eggs weeks after cure, detection of circulating antigens (CAA & CCA) in blood or urine provides evidence of an ongoing active infection, as both antigens are rapidly cleared from circulation.
Antibody tests can detect evidence of infection, but cannot distinguish current from past infection, and are not particularly useful due to cross-reactions with other helminth infections.
Treatment
Praziquantel is the drug of choice.
Prevention of schistosomiasis involves universal treatment campaigns and that has shown dramatic decrease in disease burden although it has not been helpful in eliminating the disease completely requiring repeated campaigns. Travelers can prevent schistosomiasis by avoiding bathing, swimming, wading, or other contact with freshwater in disease-endemic countries.
And finally, a mention about the World Health Organization. The World Health Organization's roadmap for eliminating neglected tropical diseases recommends targeting Schistosoma mekongi for elimination. Current strategies in affected communities include: Preventive chemotherapy targeting at-risk populations (e.g., entire villages along the Mekong) and distribution of information and education, improvements in water, sanitation, and hygiene.
Some more reading:
CDC resources: https://www.cdc.gov/schistosomiasis/resources/





.JPG)
.JPG)
.jpg)