This week's case was donated by the very astute microbiology laboratory at the MetroHealth System who detected an important - but unexpected - finding. The patient is an elderly man on inhaled bronchodilators and steroids for persistent eosinophilic asthma who presented with fever, dry cough and shortness of breath. Reverse transcription PCR (RT-PCR) tests for circulating respiratory viruses were negative. However, blood cultures grew a number of bacteria including Gram negative bacilli, and the following were noted in a stool ova and parasite exam:
An additional finding was seen on the sheep blood agar plate of the sputum culture:

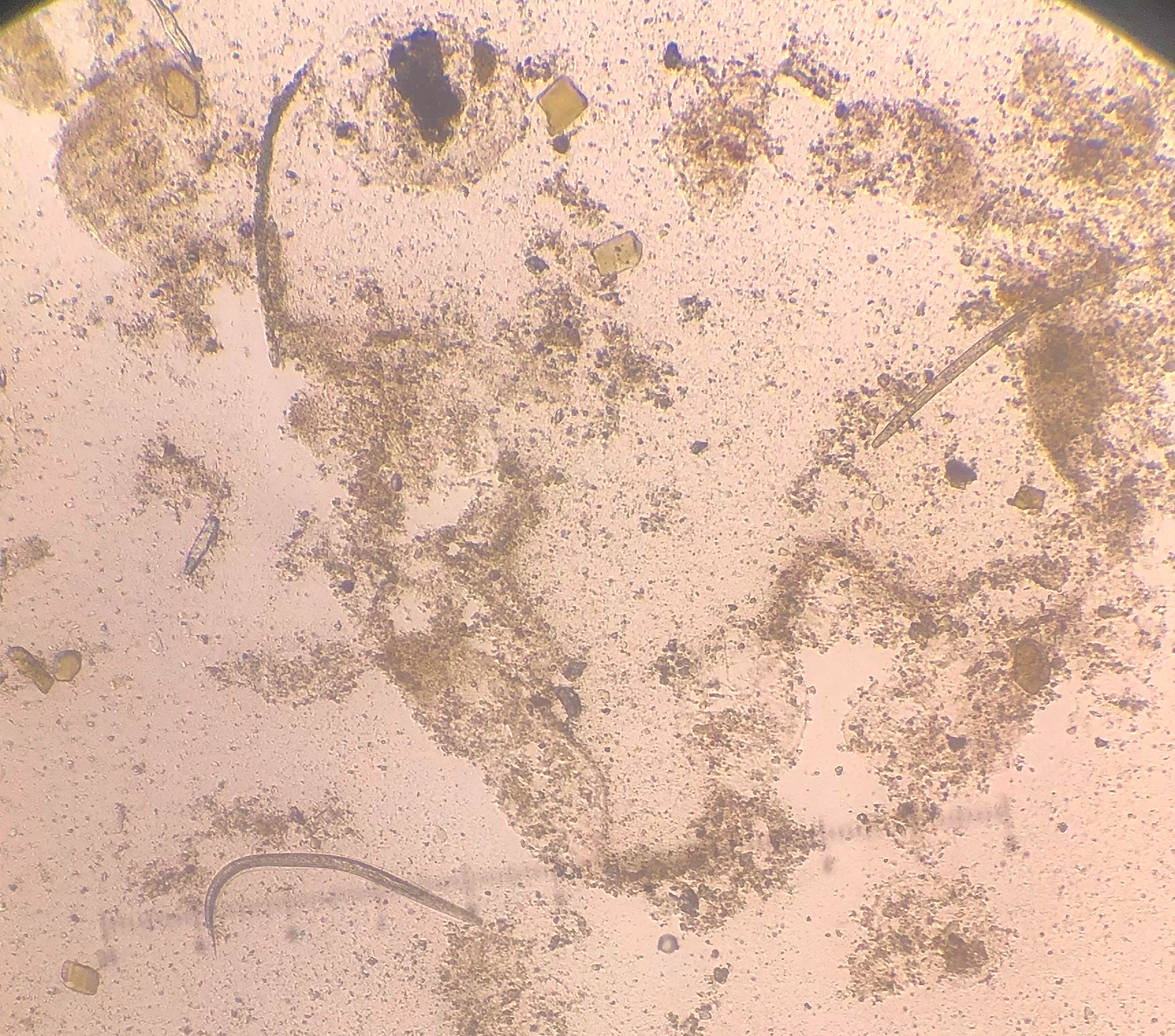
Review of the sputum showed the following:
What parasite is present here?








11 comments:
S. stercoralis since the morphology of the filariform larva consists of a notched tail. The eggs cannot be differentiated since it is similar to hookworms. The blood agar culture shows migrating S. stercoralis.
dx easy with what was given. but, i have a question regarding the workup.. I have my suspicions, but i don't want to "poison the well".... although no stranger to tropical medicine clinically, (due to humanitarian work abroad) i AM very new at formally studying this...finally getting serious re: preparing for boards....and i would greatly appreciate the full benefit of the knowledge of this blog's amazing audience...WHY was an O&P done on this patient?
Sean, steroids for persistent eosinophilic asthma who presented with fever, dry cough and shortness of breath (other common causes excluded) and Gram negative bacteraemia (with no obvious focus such as urinary tract and biliary tract) are indications to look for Strongyloides. GN bacteria 'piggy back' on the larvae as they autoinfect entering from gut into blood setting up another cycle.
Great questions Sean, which Harsha answered well. This presentation is classic for Strongyloides hyperinfection (and something that often shows up on boards). I'll just add that we owe this diagnosis initially to an astute internal medicine resident who saw the patient and ordered the O&P. The patient didn't have a recent travel history, so the lab initially cancelled the order. However, the resident called the lab to ask for the test to be done regardless, given the suspicious clinical history, and the lab ended up approving the order. Think how easily this could have been missed! Indeed, these cases are often diagnosed only at autopsy.
Strongyloides stercolaris.
An hyperinfection because this patient used corticosteroids.The use of this substance activates the larval ecdysis process, favoring the hyperinfection process. And modulates the immune response (presence bacteria)
On the blood agar photo one can see the trail of a couple of Strongyloides. Reminiscent of the cultures of Micronehaa (Pelodera) we would grow for class. This is a facultative soil nematode that generally infects skin of a variety of animals including humans.
Note eggs of Strongyloides are larvated when laid and are much smaller than morulate hookworm eggs.
I have little to say but agree with all previous comments. The case is so clinically typical. The steroid treatment exacerbates the hyperinfection. The bacteria "hitch hike" the nematode and gives the patient a secondary infection.
One good point that clinical bacteriologists need to remember is to wear gloves when reading bacti cultures, filariform nematodes are infectious, they do penetrate the skin.
Thank you Dr. Pritt for this very interesting case.
Florida Fan
Thank you all so much (and especially harsha) for your gracious replies... your elegant elucidations as "old one" might say... ;-) and i think that is what i was fishing for... a more complete H&P, and w/u for the GN bacteremia, or some other implied smoking gun.... vs "just" index of suspicion based on what was given. i wanted to make sure i wasn't missing something, vs just jumping at "key words and tricky phrases" .... it is "textbook", and i am fully expecting to encounter it on boards...easy to retro diagnose but, a small leap of logic going forward as presented...strong work and kudos to the resident! again, thank you so much for taking time to mentor me.... i am a long time fan/follower... this a great site for board prep, and especially with all of the clinical pearls dropped in the comments... you all have taught me much and i am looking forward to learning more...when i pass my boards, i'll certainly have you all to thank! please stand by for more questions in the coming months and i hope i won't be too much of a bother.... cheers!
We welcome your comments and questions Sean! Best of luck on your board prep and the exam itself. Hopefully the coming cases will be of benefit to your studies!
Strongy, where's he from?
My old friend Strongyloides!
Lee
Post a Comment