I have a fascinating parasite for the dreaded Case of the Week 666 - not a bad way to end out 2021! I promise I will start us off in 2022 with something fun.
The following was seen on a Giemsa-based stain from a liver cyst. Identification?

I have a fascinating parasite for the dreaded Case of the Week 666 - not a bad way to end out 2021! I promise I will start us off in 2022 with something fun.
The following was seen on a Giemsa-based stain from a liver cyst. Identification?
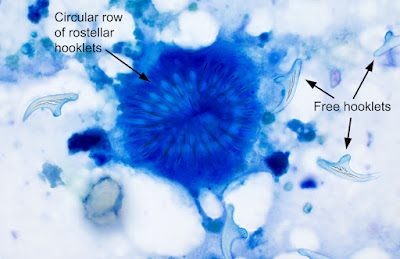
Answer to the Parasite Case of the Week 666: Echinococcus sp. degenerating protoscolex (immature scolex) and free hooklets. We can't say which species of Echinococcus is present from the image alone, but it is most likely to be E. granulosus, as this is the most common species to infect humans, and it commonly forms a liver cyst that is amenable to aspiration.
This is a beautiful example of rostellar hooklets in a protoscolex.
Here are some other great examples of Echinococcus sp. protoscoleces and hooklets in aspirate fluide from previous posts:



This week's case was made possible by BEI Resources and the NIH-NIAID Filariasis Research Reagent Resource (FR3) Center. They provided the materials and excellent instructions for this special experiment:

These black elliptical objects measure ~550-600 micrometers long, and came dried on a piece of paper towel. I added a strip of the paper towel to a Petri dish containing distilled water and waited about 30 minutes for the action to start. Here is what happened:
Here are some still shots of the action:


Answer to the Parasite Case of the Week 655: Culicidae mosquito eggs and larvae. The appearance of the eggs (darkly-colored, individual eggs, not in a raft, and without bilateral floats) is consistent with Aedes spp. Since I ordered these specifically from the FR3, I can say with certainty that these are eggs those of Aedes aegpti. I hope you all enjoyed the video of the wriggling L1 larvae!
Here's another fun case from my lab, courtesy of our awesome parasitology technical specialist, Heather Morris. The following objects were found on screening colonoscopy.



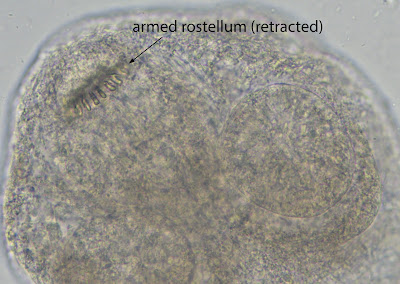
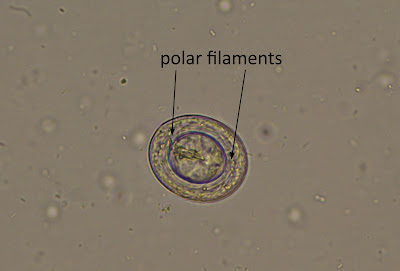
Answer to the Parasite Case of the Week 664: Hymenolepis (Rodentolepis) nana scolex and egg.
It is very unusual to see a scolex of H. nana; in my experience, it is usually only the proglottids that are removed when seen during colonoscopy. Therefore, it's a real treat to get to see the scolex in an actual clinical specimen!
Like Taenia solium and Dipylidium caninum, the scolex has an armed rostellum (i.e., protrusion with hooklets). The rostellum of H. nana is generally smaller than that of T. solium, and is often retracted.
The presence of characteristic H. nana eggs allows for definitive identification. Note the filaments emanating from each pole of the inner membrane.
This week's case was generously donated by Monica Jarvis, Lilian Flores, and the parasitology lab at the North Carolina Department of Health and Human Services. They identified the following structures in a stool wet mount. They measure approximately 160 micrometers in length. Identification?


Answer to the Parasite Case of the Week 663: Not a human parasite; "Beaver bodies".
Beaver bodies are sporocysts of the unicellular, eukaryotic protozoon, Psorospermium cf. haeckeli (Hilgendorf 1883), a parasite of crayfish. They may be seen in the stool of individuals after eating crayfish, and thus obtaining a dietary history may be helpful. Sporocysts are the host-dependent stage, and are released into the environment after the crayfish host dies. In nature, free-living amoeboids emerge from the sporocyst and are capable of infecting new crayfish.
The genus Psorospermium is located phylogenetically near the animal-fungal divergenc and was formerly thought to be an alga. Only one species (haeckeli) has been described, but molecular analysis suggests that there may be multiple species.
Psorospermium sporocysts have a distinct appearance, but may be mistaken for various helminth eggs such as those of Trichuris trichiura and Enterobius vermicularis, as well as diatoms. Fortunately, Psorospermium sporocysts can be differentiated by their large size and characteristic shape.
Here is a comparison between beaver bodies and diatoms:

This week's case is a stool specimen from a 52-year-old Bolivian farmer. He complains of intermittent right upper quadrant pain, and an abdominal CT showed edema and dilation of the bile ducts.

Identification?
Answer to the Parasite Case of the Week 662: Fasciola/Fasciolopsis/Echinostoma species eggs. The clinical history is most consistent with infection with the liver fluke, F. hepatica, rather than infection with an intestinal fluke. As mentioned by Bernardino, Florida Fan and SB, Fasciola gigantica is also in the differential diagnosis, based on the morphology of the eggs. However, it is not found in the Americas and can therefore be excluded.
Fasciola spp., Fasciolopsis buski, and Echinostoma eggs have a similar appearance, measuring up to 130-150 in greatest dimension, and having a small operculum. In particular, the eggs of Fasciola spp. and F. buski can be particularly challenging to differentiate, although the abopercular end of the former often has a roughened or irregular area. As noted by Sheldon, size matters in parasitology! The large size of these eggs allows similar appearing fluke and cestode eggs to be excluded from the differential.

Fasciola hepatica has an interesting life cycle. I would highly recommend checking out this really cool VIDEO on F. hepatica to see all of the different stages of the F. hepatica life cycle.
The following microfilariae were seen on Giemsa-stained preparations of whole blood following the Knott's concentration procedure. They are between 180 to 200 microliters in length. No travel history was initially available. Identification?




Thanks to Heather Morris for these beautiful photos.
Answer to the Parasite Case of the Week 661: Mansonella perstans microfilariae.
As many of you noted, this filarial worm has very small, unsheathed microfilariae. Note that the microfilariae are more slender than the eosinophils - and even the RBCs! That is one of the most helpful features. They also have a blunt tail, and the nuclei extend to the tip of the tail.

This week's case is another histopathology finding from an eye. The entire orbit was removed because of the presence of a parasitic cyst. You can see the digital slide HERE. Identification?
Here is a screen shot of the digital slide:

Answer to the Parasite Case of the Week 660: Cysticercus; larval form of Taenia solium
As noted by Blaine, this is "ocular cysticercosis caused by T. solium, as indicated by a single protoscolex. Coenurosis caused by a zoonotic Taenia is also a possibility, but coenuri have multiple protoscoleces, as do hydatid cysts of Echinococcus. Sparganosis is another cestode infection that can manifest in the eyes, but they do not produce protoscoleces at all." Lots of great eye puns in the comments!
Here are some of the key diagnostic features:


This week's case features a digitally-scanned section of a subcutaneous nodule from the thigh of a man living in rural Senegal. The man presented with a several month history of severe itching in his lower extremities and abdomen, accompanied with a papular skin rash and focal loss of skin pigmentation.
Here is a low power view of the skin and underlying nodule:

Answer to the Parasite Case of the Week 659: Onchocerca volvulus adult worms and microfilarie.
If you didn't already see it, check out the whole slide scanned image HERE.
In this case, you can see a large subcutaneous nodule containing the adult worms (each female with a characteristic "double barrel" uterus) and microfilariae being released into the surrounding skin.

The microfilariae are the primary source of disease, as they crawl through the skin causing intense itching and inflammatory changes. They also go to the eye and cause irreversible blindness. The latter is the reason that infection is called "River Blindness". Infection is transmitted through the bite of infected black flies (Simulium sp.) which breed in fast flowing waters.


Answer to the Parasite Case of the Week 658: Trypanosoma brucei
Given the travel history and rapid onset of symptoms, T. b. rhodesiense is the most likely parasite present. This case shows very high parasitemia with numerous trypomastigotes seen on the patient's thick blood film. Here is the corresponding thin blood film, highlighting some of the key diagnostic features:

This week's case features a Giemsa-stained thin blood film from a patient with recent travel to India. Identification? For a BONUS, can you list the different stages in images 1-4 below?




Answer to the Parasite Case of the Week 657: Plasmodium vivax
Thanks to all of the great comments on this case! There are so many classic features of P. vivax here, that it makes for a fabulous teaching slide. Florida Fan very nicely outlined all of the diagnostic features along with his thought process for coming to the final identification:
1/ The ring is fairly large, and the infected red cell is larger than the not infected. As such, there is a predilection for reticulocytes. Either P. vivax or P. ovale.
2/ The mature trophozoites are ameboid form, showing them to be highly Vivacious. More than likely P. vivax.
3/ The schizont in the third picture demonstrates more than twelve merozoites, P. ovale does not usually have that many. (on average, 8)
4/ The gametocyte in the fourth picture is not Falciform, it occupies almost the entire red cell. Though there is a little bit of fimbriation, all evidence gathered so far including the geographic area are consistent with an identification of P. vivax.
Here is a composite image of the 4 forms shown in this case:

It's time for our monthly case with Idzi Potters and the Institute of Tropical Medicine, Antwerp:
The following was seen in a urine sediment from a backpacker returning to Belgium following a 2-month's trip in Northern Senegal. During his travels, he reports being bitten by insects, drinking and eating local foods, and swimming in fresh water lakes. He is asymptomatic, but is concerned that he may has picked up a parasite along the way.
How would you interpret this finding?
Answer to the Parasite Case of the Week 656: mite, probable contaminant from the environment. Not likely of human medical significance.
As several readers noted, this mite is not one of the 2 human pathogenic mites, Sarcoptes scabei or Demodex. Instead, it is likely a mite from the environment, such as Dermatophagoides, the dust mite. The presence of many squamous epithelial cells in the background would support this idea:

You can read the following posts for more information for how to differentiate the various mites found in human specimens:
Case of the Week 634: Free-living mite found in stool
Case of the Week 196: Differentiating Sarcoptes scabei from other mites
Case of the Week 601: Key identifying features of Sarcoptes scabei
This week's case features small (~2 micrometer long), oval-shaped objects seen in a corneal scraping. Thanks to Heather for taking these beautiful images. The stain is strong trichrome (chromotrope 2R method).



What is the most likely diagnosis?
Answer to the Parasite Case of the Week 655: Microsporidia spores. Nucleic acid amplification/sequencing and/or electron microscopy is required for genus and species level identification.
Microsporidia that are commonly implicated in corneal infection include Vittaforma corneae and Encephalitozoon hellem.
As noted by Dr. Harsha Sheorey, the Ryan’s modified Trichrome stain was created by his friend and colleague, Dr Norbert Ryan. This stain has now become a standard staining technique for these organisms, and what was used in this case. The microsporidia spores stain bright red against a blue background.

This week's case is of a middle-aged man with a painful lesion on the dorsum of his foot. He recently returned from Brazil, during which he swam in the ocean, walked barefoot on the beach, and ate local foods. An excisional biopsy was performed and submitted to the clinical microbiology lab to rule out a possible parasite. The specimen received was an excised ellipse of skin on which there was a central defect measuring ~ 5 mm in diameter:





Answer to the Parasite Case of the Week 654: Tunga sp. flea
I encourage you to check out the posts in the Comments section by Kosta and Florida Fan who give us an excellent description of the taxonomy, morphology, epidemiology, and clinical presentation of this parasitic flea.
Here are some of the diagnostic features from this case:
Tunga sp. eggs measuring ~0.6 mm long:


This week's case was generously donated by Drs. Alex Fenwick and Julie Ribes at the University of Kentucky. The following structure was retrieved from bronchial washings of a patient with end-stage lung disease due to cystic fibrosis.





