Here is our last case of 2024, courtesy of Drs. Courtney Comar and Laura Lamps. The following structures were seen in tissue removed during surgery from the peritoneal cavity of a patient with volvulus of the bowel and associated inflammatory changes. On histopathology, numerous foreign body giant cells and 'pulse granulomas' were seen. What are these structures?
Monday, December 30, 2024



Sunday, December 29, 2024
Answer to Case 764
Answer to the Parasite Case of the Week 764: Artifact; not a human parasite. This material closely resembles plant spirals. This was a challenging case to be sure! However, there were a few clues that can help us out here:
First, note that the outer contour of these worm-like objects consists of spiral, refractile rings that look a bit like a 'slinky' (for those of you who remember those old toys!)

Second, I mentioned that numerous foreign body giant cells and 'pulse granulomas' were seen on histopathology. Pulse granulomas are granulomas associated with a foreign-body reaction and often contain identifiable vegetable material. The term 'pulse' refers to the edible seeds of leguminous vegetables. The presence of vegetable material elsewhere in this specimen support our diagnosis of vegetable spirals here.
For further confirmation, I turned to our friend and botany expert, Dr. Mary Parker, for her advice on this case. She indicated that we are likely seeing xylem vessels with spiral thickenings from plant vascular bundles (veins). She noted that "the simple spiral thickening in the above is typical of plant material such as young leaves (i.e. not as heavily thickened as in woody material), whereas the xylem thickenings in the colon wall are much more heavily lignified, indicating more mature plant material." She also explained that "young leaves like spinach, lettuce and parsley will all have a mixture of lightly and more-heavily thickened xylem." I remember learning about xylem and phloem back in primary school, but I never thought they would be useful in parasitology. Many thanks to Mary for her input, and kudos to Idzi for getting this case correct!
Check out the beautiful xylem spirals from this POST.
Wishing you all a very happy, healthy, peaceful, and productive new year.
Monday, December 16, 2024
Case of the Week 763
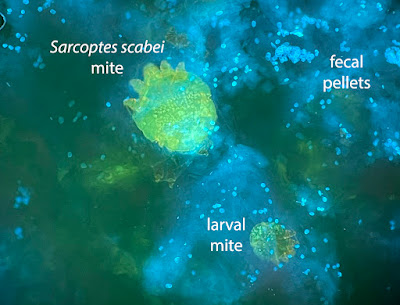
This week's case was donated by Dr. Andrew Bryan, Molly Weatherholt, Clarissa Ljungren, Bashi Ebrahimi, and Jacob Karsten. These striking images are from skin scrapings from an elderly patient with suspected superficial cutaneous fungal infection. The material was stained with Calcofluor white and examined with fluorescence microscopy. Diagnosis? What are the objects seen here - the big and little ones?



Sunday, December 15, 2024
Answer to Case 763
Answer to the Parasite Case of the Week 763: Sarcoptes scabei mites and their scybala (fecal pellets) - or, as Mike M. said - "scabies, and a lot of their poop!"
As Idzi noted, "...the small stuff on the 2nd image has the right size and the typical “puck”-shape with a dent, to be compatible with mite-droppings." However, Florida Fan also mentioned that we need to rule out small yeasts such as Malassezia spp. since they could also be present in the same slide - a great reminder!
In case you were wondering what scabies eggs looks like, here is a case that Florida Fan donated to the blog years ago:


Thanks again to Dr. Andrew Bryan, Molly Weatherholt, Clarissa Ljungren, Bashi Ebrahimi, and Jacob Karsten for donating this great case.
Tuesday, December 3, 2024
Case of the Week 762
This week's case comes from my own lab - an unexpected finding on routine colonoscopy. These beautiful photos are courtesy of Felicity Norrie. Identification?



Sunday, December 1, 2024
Answer to Case 762
Answer to the Parasite Case of the Week 762: Enterobius vermicularis male
As noted by Idzi Potters, "The ribbed cephalic alae are typical for an Enterobius vermicularis adult. The curved tail and spicula (although retracted) point towards an adult male." These features can be easily appreciated in the below composite image. Thanks again to Felicity for the beautiful photographs!

Others asked about the clinical significance of this finding. In this case, the patient was asymptomatic and there was likely no clinical relevance. This is not surprising, as enterobiasis is frequently asymptomatic,. However, it is likely that this patient was treated to eliminate the chance of him serving as a reservoir for infection.
Monday, November 18, 2024
Case of the Week 761
This week's case was generously donated by Drs. Taylor Williams and Karl Kirby. The following object was passed per rectum by a child living in the Western US without travel outside of the country. The family also does not report any international travel. What is your differential diagnosis?
.jpg)
.jpg)
.jpg)
Sunday, November 17, 2024
Answer to Case 761
Answer to the Parasite Case of the Week 761: Diphyllobothrium/Dibothriocephalus/Adenocephalus (diphyllobothriid) species. These worms are commonly referred to as the broad fish tapeworm based on the fact that their proglottids are broader than they are tall and they are acquired through eating undercooked fish. The diphyllobothriid tapeworms have a very characteristic 'rosette-shaped' central uterus which we can see here:
_answer.jpg)
This picture also nicely shows the craspedote nature of the proglottids, characteristic of the diphyllobothriid tapeworms. The term craspedote refers to the overlapping arrangement of the proglottids - like shingles or tiles. This feature, along with the uterine structure, is helpful in differentiated the diphyllobothriid tapeworms from Taenia species.
Thanks again to Dr. Taylor Williams and Karl Kirby for donating this highly educational case.
Monday, November 11, 2024
Case of the Week 760
This week's case was generously donated by Dr. Adrienne Showler. The patient is an immunocompromised middle-aged man from El Salvador who presented with vomiting, diarrhea, and weight loss. The following are hematoxylin and eosin-stained images of the duodenal biopsy. What is your diagnosis? What are the structures shown?
%5B64%5D.jpg)
%5B99%5D.jpg)
Sunday, November 10, 2024
Answer to Case 760
Answer to the Parasite Case of the Week 760: Strongyloides stercoralis larvae, eggs, and an adult female in the small intestine. This is an important finding as the patient might be at risk for life-threatening hyperinfection syndrome. Some eggs are unembryonated, whereas others have matured and contain larvae.
%5B99%5D.jpg)
The differential diagnosis of adult nematodes, larvae, and eggs within the intestinal mucosa is limited. Capillaria (=Paracapillaria) philippinensis can have a similar appearance, but Capillaria eggs have a striated wall and bipolar plugs which allow for their differentiation from the thin-walled eggs of S. stercoralis. Also, both male and females are present in C. philippinensis, whereas only females are seen in S. stercoralis infection.
Thanks again to Dr. Showler for donating this great teaching case!
Monday, October 28, 2024
Case of the Week 759
This week's case is very appropriate for Halloween! The following object was found attached to the wall of the terminal ileum during screening colonoscopy. It was removed and sent to the parasitology laboratory for identification where it was cleared and mounted on a glass slide. It is approximately 1-cm long. Images by Heather Morris.



What is your diagnosis? The answer will be posted on Halloween, courtesy of Dr. Jacob Rattin.
Sunday, October 27, 2024
Answer to Case 759
Answer to the Parasite Case of the Week 759: Female Ancylostoma duodenale
The following explanation is by the outstanding PGY-2
pathology resident, Dr. Jacob Rattin:
In humans, intestinal hookworm infection is predominantly caused
by Ancylostoma duodenale, Necator americanus, and A.
ceylanicum. Adult hookworms live in the small intestine (typically the
distal jejunum) and use specially-adapted mouthparts to attach to the intestinal mucosa
and feast upon the host’s blood (creepy!). Females release unembryonated eggs
into the feces where they mature in the soil and then release larvae. These
infectious larvae can pierce human skin and travel in the blood to the lungs
where they can penetrate alveoli and make the ascent up the bronchial tree and
into the pharynx. After being swallowed, they make their way to the small
intestines where they attach. Chronic infection results in iron-deficiency
anemia and malnutrition (dreadful!). Rarely, heavy infection can result in
death, especially in infants.
The sizes and morphology of rhabditiform larvae, filariform
larvae, and adults differ. For ease of comparison and reference, a table has
been made for Ancylostoma duodenale.
|
Stage |
Size |
Morphology |
|
Rhabditiform
(L1) larvae |
250-300 µm
long |
- Long buccal
canal - Inconspicuous
genital primordium - Can occasionally
be seen in stool when there is a delay in processing (see
COTW 757), and need to be distinguished from L1 Strongyloides
stercoralis larvae. |
|
Filariform
(L3) larvae |
500-700 µm long |
- Ensheathed,
pointed tail |
|
Adults |
Females: 10-15
mm long Males: 8-12
mm long |
- Sharp teeth - the male
tail has a large fan-like copulatory bursa, while the female has a pointed
tail. |

The buccal capsule shows the characteristic cutting teeth in
this image of Ancylostoma duodenale, which differentiates it from
Necator, which has cutting plates. The teeth of A. ceylanicum have
a similar appearance to that of A. duodenale but have larger from teeth.
This scary appearance really shows how A. duodenale is
like a real vampire!

For extra tricks and treats, check out my past parasite-themed Halloween images:
https://www.parasitewonders.com/parasites/fun-parasite-images

Wednesday, October 16, 2024
Case of the Week 758
This week's case was generously donated by Professor Philippe Poirier, Dr. Céline Nourrisson, and Dr. Maxime Moniot, Parasitology-Mycology Department, National Reference Centre for Cryptosporidiosis, Microsporidia and Other Digestive Protozoa, Clermont-Ferrand Teaching Hospital, France.
The following objects were seen in a stool specimen from a patient with diarrhea.
Concentrated wet prep:



Giemsa-based stain:


Many were still moving!
Diagnosis?
Tuesday, October 15, 2024
Answer to Case 758
Answer to the Parasite Case of the Week 758: Balantioides coli
This protozoan is the largest to infect humans, and is the only human ciliated parasite. It has circumferential cilia and a large macronucleus (not well appreciated in the slides here) which give it a striking appearance. Note the characteristic 'boring' (rotary) motility - nothing boring about this parasite!

Thanks again to our contributors, Professor Philippe Poirier, Dr. Céline Nourrisson, and Dr. Maxime Moniot, Parasitology-Mycology Department, National Reference Centre for Cryptosporidiosis, Microsporidia and Other Digestive Protozoa, Clermont-Ferrand Teaching Hospital, France.
Wednesday, October 9, 2024
Case of the Week 757
The following objects were seen in a fresh stool specimen collected at a field station in Uganda. The objects are approximately 280 µm long and no longer motile upon examination. What is your identification?


Sunday, October 6, 2024
Answer to Case 757
Answer to Parasite Case of the Week 757: Hookworm rhabditiform (L1) larvae
Many of you questioned if these were Strongyloides stercoralis larvae, since this parasite most often presents with L1 larvae in stool. In comparison, hookworm larvae are rarely seen in stool, and only when there is a prolonged period between specimen collection and placement in fixative (as occurred in this case). Fortunately, hookworm L1 larvae can be differentiated from those of S. stercoralis L1 larvae by several morphologic features:
- Hookworm larvae (Ancylostoma duodenale and Necator americanus) have a long buccal cavity and an inconspicuous genital primordium.
- S. stercoralis larvae have a short buccal cavity and conspicuous genital primordium. (Think Strongyloides = Short)
Note the long buccal cavity in this case:

Here is a nice image from Case of the Week 459 showing the two L1 larvae side-by-side:

While I tried to provide you some clues to the diagnosis (received fresh, not in preservative, and larvae were no longer motile upon examination), this was definitely a challenging case!
Thanks to everyone who wrote in with their thoughts.
Tuesday, September 3, 2024
Case of the Week 756
This week's case was generously donated by Dr. Michal Kamionek. The following worms were identified on routine screening colonoscopy in the small and large intestine. A portion of one worm was submitted to anatomic pathology for examination, and the section is shown below. What is your identification?


Monday, September 2, 2024
Answer to Case 756
Answer to the Parasite Case of the Week 756: Cestode, most likely Rodentolepis (Hymenolepis) nana.
The colonoscopy image shows numerous short white worms attached to the intestinal mucosa, raising the possibility of a small nematode (e.g., hookworm, Trichuris trichiura) or cestode. Fortunately, the histopathology allows us to easily differentiate between these two categories as you can see the characteristic cestode tegument, beginning of proglottids, and what appear to be a rostellum and two of the four suckers on the scolex.

As noted by Idzi, "Histo picture in fact looks like a VERY angry parasite… frightening… 😅". I agree! Can you all see it?

Monday, August 19, 2024
Case of the Week 755
This week's case features some objects on unstained wet preparations of whole blood. What are we seeing here? How do you process blood specimens in your laboratory for this type of organism?
Sunday, August 18, 2024
Answer to Case 755
Answer to the Parasite Case of the Week 755: microfilariae; permanent staining needed for further identification.
I'd like to give a giant shout out to the Filariasis Research Reagent Resource Center (FR3) which provided this specimen to me for a course I was teaching - the first annual Mayo Clinic Parasitology Workshop. The live microfilariae were a big hit with my course attendees, so I wanted to share the specimen with all of you as well! This particular sample contained Brugia pahangi (orderable through BEI: NR-48896).
Thanks to all of you who wrote in to share your diagnostic protocols for the microfilariae. In my laboratory, we screen all Giemsa-stained thick and thin blood films for microfilariae using the 10x objective before going to higher power. However, like Florida Fan, we offer a specific test for microfilariae when suspected clinically. For the microfilariae test, we request that blood be submitted in 3.2% sodium citrate (light blue topped tube) and then perform a Knott's concentration. We no longer examine fresh wet preps of blood due to the concern for infectious diseases (so seeing the live microfilariae in this 'safe' NIH sample was a real treat for us). The Knott's involves the addition of 2% formalin to the blood which lyses the RBCs and make the microfilariae easier to identify. We then centrifuge the specimen and make Giemsa-stained, methanol-fixed smears for examination.
You can read more about the human infecting microfilariae found in blood in a paper I wrote with Blaine Mathison and Marc Couturier HERE. There is a nice algorithm for differentiating the various species. Enjoy!
Tuesday, August 6, 2024
Case of the Week 754
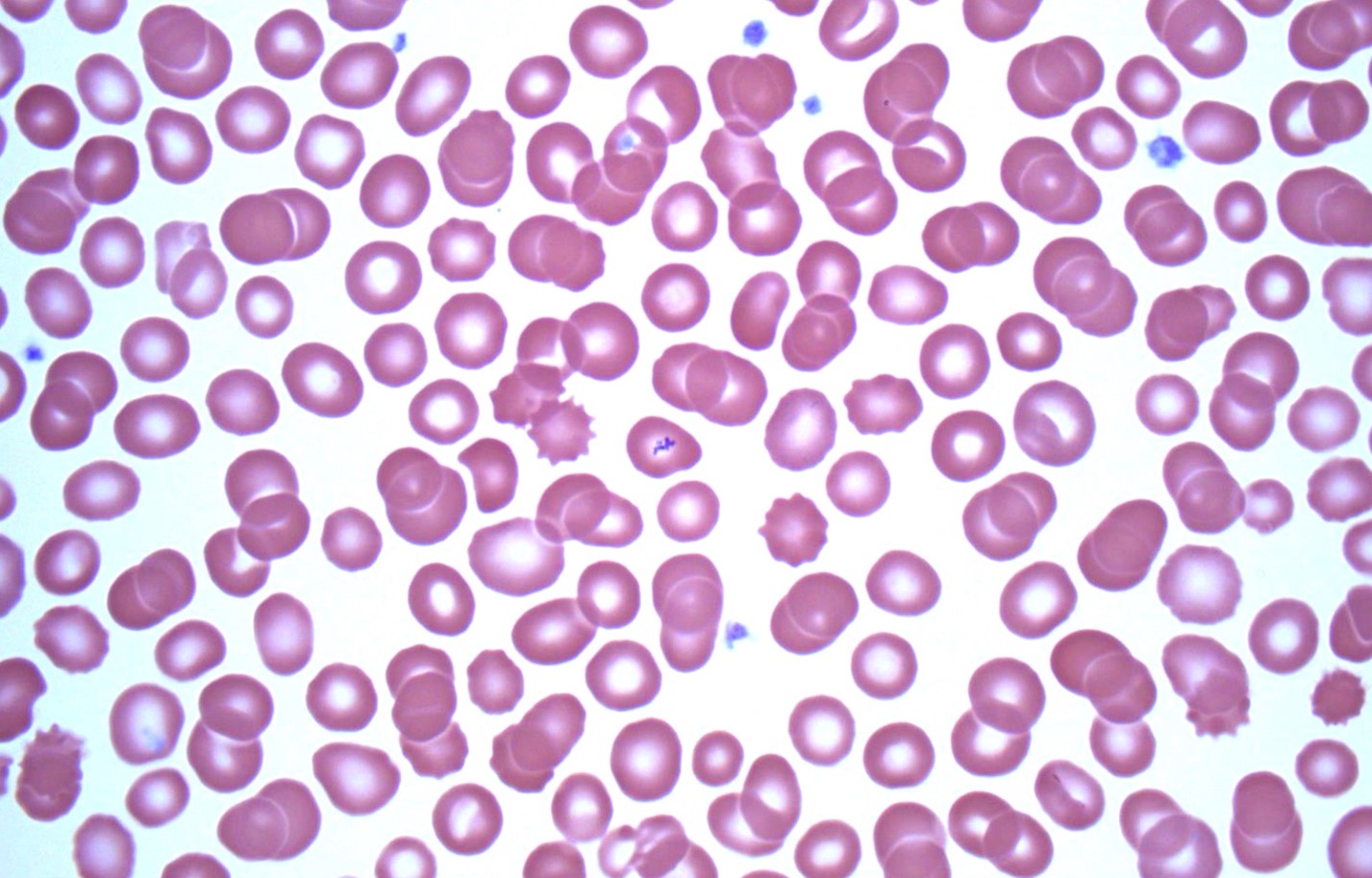
This week's case was generously donated by Dr. Jacob Rattin. The following objects were seen from Wright-stained thin blood films taken from a middle-aged woman with unexplained fevers. What is your diagnosis?



Monday, August 5, 2024
Answer to Case 754
Answer to Parasite Case of the Week 754: Platelets overlying RBCs, an intraerythrocytic blood parasite mimic. Many thanks to Dr. Jacob Rattin who donated this case and provided the following helpful explanation.
Normal platelets are 1.5-2.5 μm in diameter and are morphologically round-to-oval and granular (Figure 1, arrowheads).

On Wright stain they are usually blue/purple and on Giemsa stain they are normally pink/purple. As seen in Figures 1 through 4 (arrows), platelets can overly red blood cells (RBCs), mimicking a blood parasite (e.g., Babesia or Plasmodium). In Figure 5, the green arrow is pointing to stain precipitate overlying an RBC.




Helpful morphologic clues to differentiate this pitfall from a true parasite are the following:
1. Platelets overlying RBCs often have a “halo” around them which is likely from it pressing down upon the RBC, which signifies it is not actually intraerythrocytic.
2. The platelets lack any definitive morphology of a parasite.
3. Other normal platelets in the field should resemble the platelet/s overlying the RBC (which is apparent in Figures 1 through 5).
4. As always, clinical information integration is crucial! Checking the patient’s medical and travel history can aid in the differential diagnosis.
Subscribe to:
Comments (Atom)


